

Understanding Neuralink's Future
*That* 8 hour podcast. Where's my Electronic Caffeine?


On August 2, 2024, Lex Fridman dropped his longest ever podcast, an 8 hour conversation with the Neuralink executive team.
Through frank and freewheeling conversations with Elon Musk (Founder and CEO), DJ Seo (COO & President), Dr. Matthew MacDougall (Head Neurosurgeon), Bliss Chapman (Brain Interface Software Lead) and Noland Arbaugh (First Neuralink User), Lex serves up a buffet of topics and tangents related to BCI and far beyond.
What follows is a curated summary for the busy reader, organized topically for easy reference. Huge shout out to Lex for publishing the conversation and the full transcript online.
This filters out (most of) the speculative and philosophical discussions, including Lex’s Ayahuasca dragons and intergalactic travels, as well as hours and hours of detailed technical explanations, historical and academic context for BCI, and Musk’s unfiltered profundities on “truth,” talking to trees, politics, AGI overlords, and more.
Instead, scroll on for key neurotechnology topics with some light analysis of commercial, product, regulatory, or go- to-market implications for Neuralink and the rest of the BCI field.
Key Updates & Claims
Neuralink has implanted their second patient. Musk: “So far, so good. It looks like we’ve got, I think, on the order of 400 electrodes that are providing signals.” (note this interview was published on August 2nd, 2024)
See my earlier note for added context about Neuralink’s solution to the thread retraction issue in their first patient, Noland Arbaugh.
Their goal is 10 patients by end of year: Musk: “We’re hoping to do 10 by the end of this year, total of 10. So, eight more”
Multiplied Channel Growth: The number of channels in Neuralink’s device will increase from the current count of 1,024.
DJ Seo: “So for next versions of the implant, the key metrics that we’re looking to improve are number of channels, just recording from more neurons. We have a pathway to actually go from currently 1000 to hopefully 3000, if not 6,000 by end of this year…And then end of next year we want to get to even more. 16,000.”BCI Performance and Usability: Musk: “Well, we feel pretty confident that I think maybe within the next year or two, that someone with a Neuralink implant will be able to outperform a pro gamer…because the reaction time would be faster.”
When can an average person get a Neuralink? According to Musk: “Probably less than 10 years.”
Potential future use cases covered in this conversation include vision restoration and spinal cord stimulation. Other applications were discussed more hypothetically, like “electronic caffeine.”
What else did they cover? A lot. Specific discussions curated below include:
The n1 Implant: Explantation, Upgrading, and Multiple Implants
The r1 Robot: Computer Vision for sewing electrodes into the brain
Bits Per Second: Present & Future of this interesting metric
Read Vs Write: Restoring Vision, Other Stimulation, Enhancement
BCI & UX: Usability of BCI is paramount
Analyst Summary: Reading between the lines and speculating a bit…
Before we dive in: If you’ve read my writing before you’ll know I don’t meet the eligibility criteria for being a Neuralink superfan. But the Elon effect is real, and listening to this dialogue gave me a bigger appreciation for why he has millions of supporters (and critics) worldwide. While he is clearly a smart chap, I personally found his views to be the most boring and unhinged, from a pure BCI standpoint.
But his team is world class. After spending days last week listening and re-listening to portions of this talk, I came away with more respect for the expertise and passion of the other executive leaders at Neuralink, and a deeper understanding of their unique approach (along with many open questions about their commercial future.)
A portion of these curated notes is free before the paywall. If you’re a free-tier reader, Lex’s transcript is well-organized and 100% free, so please go there, read and be merry.
The n1 Implant
Here are Musk and Seo talking generally about Brain-Computer Interfaces.
Musk: “…It’s really a generalized input-output device. It’s reading electrical signals, and generating electrical signals, and I mean, everything that you’ve ever experienced in your whole life, smell, emotions, all of those are electrical signals.”
Seo: “As much as you’re learning to use that thing, that thing is also learning about you. Our model’s constantly updating the way to say, “Oh, if someone is thinking about this sophisticated forms of spiking patterns, that actually means to do this.”
Here’s what an “n1” looks like, with some technical specs from DJ Seo:

Seo: “So the current instantiation of the device has 64 threads, and each thread has 16 electrodes for a total of 1,024 electrodes that are capable of both recording and stimulating. And the thread is basically this polymer-insulated wire. The metal conductor is the kind of a tiramisu cake of ti, plat, gold, plat, ti and they’re very, very tiny wires. Two micron in width. So two one-millionth of meter.”
Seo: “So each of these threads are…16 micron in width, and then they taper to 84 micron, but in thickness they’re less than five micron. And in thickness it’s mostly a polyimide at the bottom and this metal track and then another polyimide. So two micron of polyimide, 400 nanometer of this metal stack and two micron of polyimide sandwiched together to protect it from the environment that is a 37 degrees C bag of salt water.
Seo: “it’s three or four millimeters from the surface just because the span of the electrode, those 16 electrodes that we currently have in this version, spans roughly around three millimeters. So we want to get all of those in the brain.”

A screengrab from an earlier Neuralink presentation on their X feed, which discussed deeper placement of electrodes (up to 5.5.mm) to mitigate thread retraction issues. Note: this wasn’t really discussed specifically in the pod.

Explantation
Seo: “In the first three months or so after the surgery, there’s a lot of tissue modeling that’s happening. Similar to when you got a cut, you obviously start over first couple of weeks or depending on the size of the wound, scar tissue forming, there are these contractive, and then in the end they turn into scab and you can scab it off. The same thing happens in the brain. And it’s a very dynamic environment. And before the scar tissue or the neo membrane or the new membrane that forms, it’s quite easy to just pull them out. And there’s minimal trauma that’s caused during that.
Once the scar tissue forms, and with Noland as well, we believe that that’s the thing that’s currently anchoring the threads. So we haven’t seen any more movements since then. So they’re quite stable. It gets harder to actually completely extract the threads. So our current method for removing the device is cutting the thread, leaving the tissue intact, and then unscrewing and taking the implant out. And that hole is now going to be plugged with either another Neuralink or just with…a plastic based cap.
Lex: Is it okay to leave the threads in there forever?
DJ Seo: “Yeah, we think so. We’ve done studies where we left them there and one of the biggest concerns that we had is, do they migrate and do they get to a point where they should not be? We haven’t seen that. Again. Once the scar tissue forms, they get anchored in place. And I should also say that when we say upgrades, we’re not just talking in theory here, we’ve actually upgraded many, many times. Most of our monkeys or non-human primates, NHP, have been upgraded. Pager, who you saw playing mind pong has the latest version of the device since two years ago and is seemingly very happy and healthy and fat.
Upgrading Implants
There are two ways to talk about “upgrading” implants: Software and hardware.
Noland Arbaugh’s thread retraction issue involved upgrading the software to change the recording interpretation:
Chapman: “So we just did an over-the-air software update to his implants, same way you’d update your Tesla or your iPhone. And that firmware change enabled us to record averages of populations of neurons nearby individual electrodes. So we have less resolution about which individual neuron is doing what, but we have a broader picture of what’s going on nearby an electrode overall. And that feedback loop, basically as Noland described it, it was immediate when we flipped that switch. I think the first day we did that, you had three or four BPS right out of the box, and that was a light bulb moment for, okay, this is the right path to go down.
For future hardware upgrades, the device may become more modular:
Seo: “So you can’t actually separate the thing out, but you can imagine having two part implant, bottom part that is the thread that are inserted that has the chips and maybe a radio and some power source. And then you have another implant that has more of the computational heavy load and the bigger battery. And then one can be under the dura, one can be above the dura being the plug for the skull. They can talk to each other, but the thing that you want to upgrade, the computer and not the thread, if you want to upgrade that, you just go in there, remove the screws, and then put in the next version. And you’re off the… It’s a very, very easy surgery too. You do a skin incision, slip this in, screw. Probably be able to do this in 10 minutes.
Seo: “So for next versions of the implant, the key metrics that we’re looking to improve are number of channels, just recording from more and more neurons. We have a pathway to actually go from currently 1000 to hopefully 3000, if not 6,000 by end of this year. And then end of next year we want to get to even more. 16,000.”
Multiple Implants
Seo: “That’s the goal. That’s the goal. Yeah. I mean, our monkeys have had two neural links, one in each hemisphere. And then we’re also looking at potential of having one in motor cortex, one in visual cortex and one in wherever other cortex. And we talk about building a generalized neural interface to the brain. And that also is strategically how we’re approaching this with marketing and also with regulatory, which is, hey, look, we have the robot and the robot can access any part of the cortex. Right now we’re focused on motor cortex with current version of the N1 that’s specialized for motor decoding tasks. But also at the end of the day, there’s a general compute available there.”
The r1 Robot

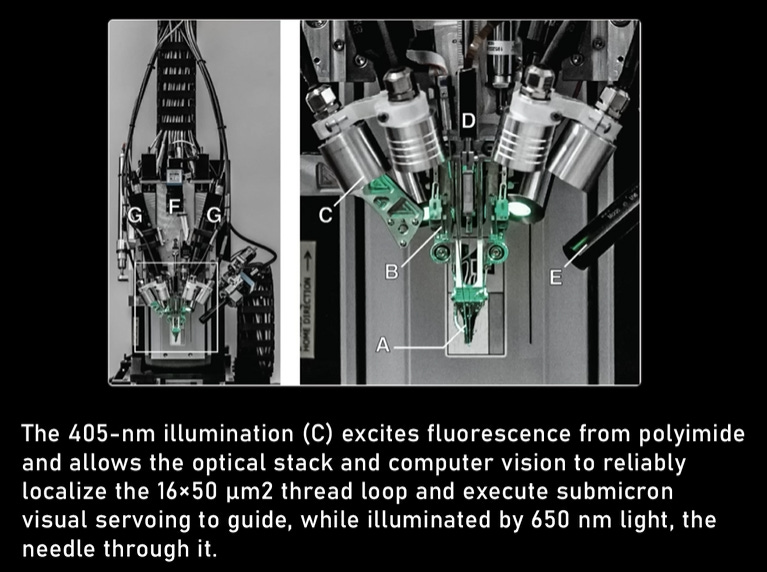
Seo: “There are other reasons for why we built the robot, and that is ultimately we want this to help millions and millions of people that can benefit from this. And there just aren’t that many neurosurgeons out there. And robots can be something that we hope can actually do large parts of the surgery. But the robot is this entire other sort of category of product that we’re working on. And it’s essentially this multi- axis gantry system that has the specialized robot head that has all of the optics and this kind of a needle-retracting mechanism that maneuvers these threads via this loop structure that you have on the thread.”

Seo: “Our robot is quite heavy, our current version of it. I mean, it’s like a giant granite slab that weighs about a ton, because it needs to be sensitive to vibration, environmental vibration. And then as the head is moving at the speed that it’s moving, there’s a lot of motion control to make sure that you can achieve that level of precision. A lot of optics that zoom in on that. We’re working on next generation of the robot that is lighter, easier to transport. I mean, it is a feat to move the robot to the surgical suite.”
McDougall, on surgical workflow: “I’ll make a little cut in the skin, we’ll flap the skin open, just like kind of opening the hood of a car, only a lot smaller, make a perfectly round one inch diameter hole in the skull, remove that bit of skull, open the lining of the brain, the covering of the brain, it’s like a little bag of water that the brain floats in, and then show that part of the brain to our robot. And then this is where the robot shines.”
MacDougall: “It can come in and take these tiny, much smaller than human hair, electrodes and precisely insert them into the cortex, into the surface of the brain to a very precise depth, in a very precise spot that avoids all the blood vessels that are coating the surface of the brain. And after the robot’s done with its part, then the human comes back in and puts the implant into that hole in the skull and covers it up, screwing it down to the skull and sewing the skin back together. So the whole thing is a few hours long. It’s extremely low risk compared to the average neurosurgery involving the brain that might, say, open up a deeper part of the brain or manipulate blood vessels in the brain.”
MacDougall: “an MD needs to be in charge of all of the medical decision-making throughout the process, I unscrubbed from the surgery after exposing the brain and presenting it to the robot and placed the targets on the robot software interface that tells the robot where it’s going to insert each thread. That was done with my hand on the mouse, for whatever that’s worth.”
Lex: So the robot with computer vision provides a bunch of candidates and you kind of finalize the decision.
MacDougall: “Right. The software engineers… provided an interface where you can essentially use a lasso tool and select a prime area of brain real estate, and it will automatically avoid the blood vessels in that region and automatically place a bunch of targets. That allows the human robot operator to select really good areas of brain and make dense applications of targets in those regions, the regions we think are going to have the most high fidelity representations of finger movements and arm movement intentions.”
(see below for thoughts on the Robot variable in Neuralink’s broader go to market equation)
To continue reading, please consider upgrading (group discounts available) or try our referral program. Hit reply with any questions.
